 |
|
پروفسور محمد حسین سلطان زاده
استاد
دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
اقای دکتر
نادر ممتازمنش
فوق تخصص خون اطفال
عضو هیئت علمی دانشگاه
به
اتفاق اعضای هیئت علمی بیمارستان
لقمان
معرفی کیس:
دکتر زندی
رزیدنت بیمارستان لقمان
دکتر فائقه علی زاده
رزیدنت بیمارستان مفید
دکتر سید رامین مدنی
رزیدنت بیمارستان امام حسین
دکتر
نوید نمازی رزیدنت بیمارستان شهدا
|
اقای دکتر
نادر ممتازمنش
فوق تخصص خون اطفال
عضو هیئت علمی دانشگاه
به
اتفاق اعضای هیئت علمی بیمارستان
لقمان

پاسخ :
تشخيص هاي افتراقي:
كودك در
اولين مراجعه تب و گلودرد داشته است و با مراجعه سرپايي به پزشك و تشخيص فارنژيت
استرپتوكوكي پني سيلين دريافت ميكند ولي تب بيمار قطع نمي شود. از بيمار
CBC
و ESR
چك ميشود كه نشانگر لكوسيتوز، نوتروپني و
ESR
بالا مي باشد.
نوتروپني به عنوان يك علامت آزمايشگاهي بيمار جهت برخورد تشخيصي
با بيماري وي انتخاب مي گردد.
در شيرخوران
از 2 هفتگي تا يكسالگي تعداد مطلق نوتروفيل (ANC)كمتر
از 1000
cells/mm3
و پس از اين سن كمتر از 1500
cells/mm3
نوتروپني تلقي مي گردد. البته اين عدد مربوط به سفيد پوستان است
و در سياه پوستان تعداد200-600/mm3
كمتر از آن مي باشد .
در بررسي
علل نوتروپني به دو گروه اصلي از عوامل برخورد ميكنيم . در گروه اول نقائص داخلي
(Intrinsic Defects
)
قرار مي گيرند و شامل بيماري هايي مانند ديس ژنزي رتيكولر، نوتروپني سيكليك،
نوتروپني شديد مادرزادي (.Kostmanns
Syn)
،
سندرم
شواخمن
–
دياموند ، چدياگ –هيگاشي،
نوتروپني فاميليال خوش خيم و آنميهاي آپلاستيك ( مادرزادي يا اكتسابي ) است.
در اين
كودك با توجه به اينكه قبل از اين بيمار مشكل مهمي دال بر نوتروپني نداشته است و
بعدا" هم با درمان مشكل نوتروپني وي برطرف شده است اين علل مطرح نميشود.
در گروه دوم
عوامل خارجي (Extrinsic
Factors
)
قرار ميگيرند و شامل مواردي مانند عفونت، داروها، بيماري ها وعلل اتوايمون،
نوتروپني همراه بيماريهاي متابوليك، كمبودهاي تغذيهاي، پركاري طحال و انفيلتراسيون
مغز استخوان است.
شايعترين
علت نوتروپني گذرا در كودكان عفونتهاي ويروسي است. ويروسهايي كه بطور شايع نوتروپني
ايجاد مي كنند عبارتند
از
EBV, CMV
،
هپاتيتA
وB
، HIV
، انفلوانزاي A
و
B
، سرخك، RSV،
پارو ويروس B19
، سرخجه و آبله مرغان. در عفونت هاي ويروسي نوتروپني در 24 تا 48
ساعت اول بيماري ايجاد ميشود و ممكن است 3تا 6 روز باقي بماند. همچنين
عفونتهايي مانند تيفوئيد، پاراتيفوئيد، سل، بروسلوز، تولارمي و عفونتهاي باكتريايي
هم ميتوانند با نوتروپني همراه باشند. سپسيس از علل جديتر نوتروپني است كه بطور
شايعتر در عفونتهاي باكتريايي نوزادان مشاهده مي گردد.
بيمار ما با تب
و ESR
بالا مراجعه نموده است. علائم باليني بيمار و
ESR
خيلي بالا به ضرر عفونتهاي ويروسي است و با عنايت به شرح حال و
اتفاقات بعدي و بخصوص
CBC
بعدي كه نوتروفيل را صفر گزارش كردهاند و كودك دچار پان سيتوپني شده است بدون
اينكه علائم سپسيس شديد را نشان دهد در نتيجه علل عفوني براي ايجاد نوتروپني بطور
اوليه در اين بيمار مطرح نميشود.
با در نظرگرفتن
پان سيتوپني در مراجعه سوم كودك و بزرگي كبد و طحال انفيلتراسيون مغز استخوان در
راس تشخيصها قرار ميگيرد كه ميتواند به علت بدخيميها ( لوسمي، لنفوم و تومورهاي
ساليد ) ، بيماريهاي گرانولوماتو، بيماريهاي ذخيرهاي ليزوزومي و يا استئوپتروزيس
باشد. راديوگرافي ريه شواهدي دال بر استئوپتروزيس را نشان نميداد و براي تشخيص
قطعي بقيه موارد انجام آسپيراسيون مغز استخوان ضروري مي شود. البته با توجه به
اندازه كبد و طحال ،شيوع بيماري ها ، سابقه فردي و خانوادگي بيمار ومشاهده سلولهاي
لنفوسيت نارس در خون محيطي در اين كودك تشخيص اول
(ALL)
Acute
Lymphoblastic Leukemia
بود
كه بررسي موفولوژي مغز استخوان و
CD
ماركرهاي سلولهاي مغز استخوان آن را تائيد كرد و كودك با اين تشخيص تحت شيمي درماني
قرار گرفت.
سير بيماري:
كودك در طول
قسمت اعظم درمان اينداكشن هم نوتروپني داشت ولي در پايان درمان اينداكشن
مغزاستخوان به رميسيون كامل رفت و
CBC
طبيعي
شد.
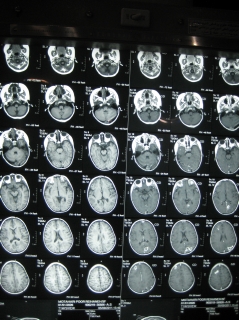
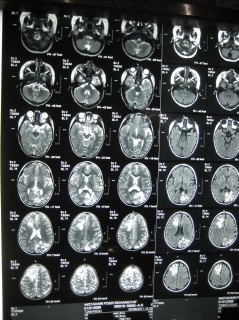
كودك در اوايل
شيمي درماني مرحله
Consolidationدچار
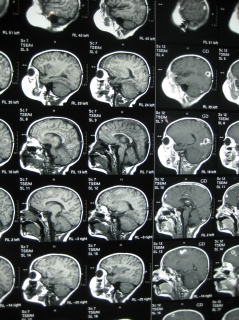
تشنج ميشود كه در بررسي تصويربرداري(MRI)
از مغز
متوجه ضايعاتي در نسج مغز همراه ادم ميشويم.
Intra axial mass lesion with mild
vasogenic edema and hemorrhage )
(
احتمال درگيري
لولميك CNS
و يا عفونت مطرح ميشود. كودك تب واضح نداشته و بررسي
CSF
هم نرمال بوده است. باتوجه به زمان بروز اين ضايعات و طبيعي بودن
CSF
درگيري لوكميك CNS
براي كودك بسيار كمتر مطرح است و درگيري عفوني
CNS
و از
جمله عفونتهاي قارچي در راس تشخيصها قرار ميگيرد. براي بيمار درمان آنتي بيوتيكي
شروع ميشود. و نمونه برداري از ضايعات مغزي با استفاده از تكنيك استرئوتاكسي در
بيمارستان شهداي تجريش انجام ميشود. تشخيص پاتولوژيست باتوجه به مورفولوژي ضايعات
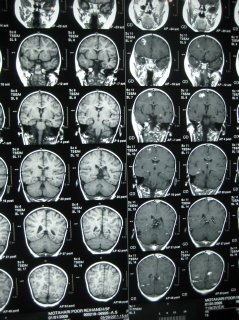
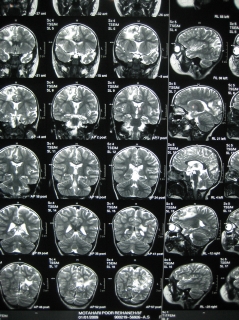
عفونت با آسپرژيلوس گزارش ميشود. براي بيمار درمان با آمفوتريسين
B
داخل وريدي و Vuriconazole
خوراكي انجام ميشود كه با بهبودي قابل توجه علائم باليني ضايعات
مغزي در MRIپس
از دوماه از درمان همراه است.
تشخيص نهايي
:
(ALL)
Acute
Lymphoblastic
Leukemia
همراه با
آسپرژيلوزيس
CNS
عکسهای بیمار
بعد از درمان
معرفی کیس:
دکتر زندی
رزیدنت
بیمارستان لقمان

تشخیص های افتراقی:
دکتر فائقه علی زاده
رزیدنت
بیمارستان مفید

دکتر سید رامین
مدنی
رزیدنت بیمارستان امام حسین

دکتر
نوید نمازی
رزیدنت بیمارستان شهدا

دکتر فائقه علی زاده
رزیدنت
بیمارستان مفید
Problem List
Recurrent Fever
Neutropenia
Hepatomegaly
Elevation of ESR
Abcess & Multiple rim enhancing lesions in Brain
Low serum IgM
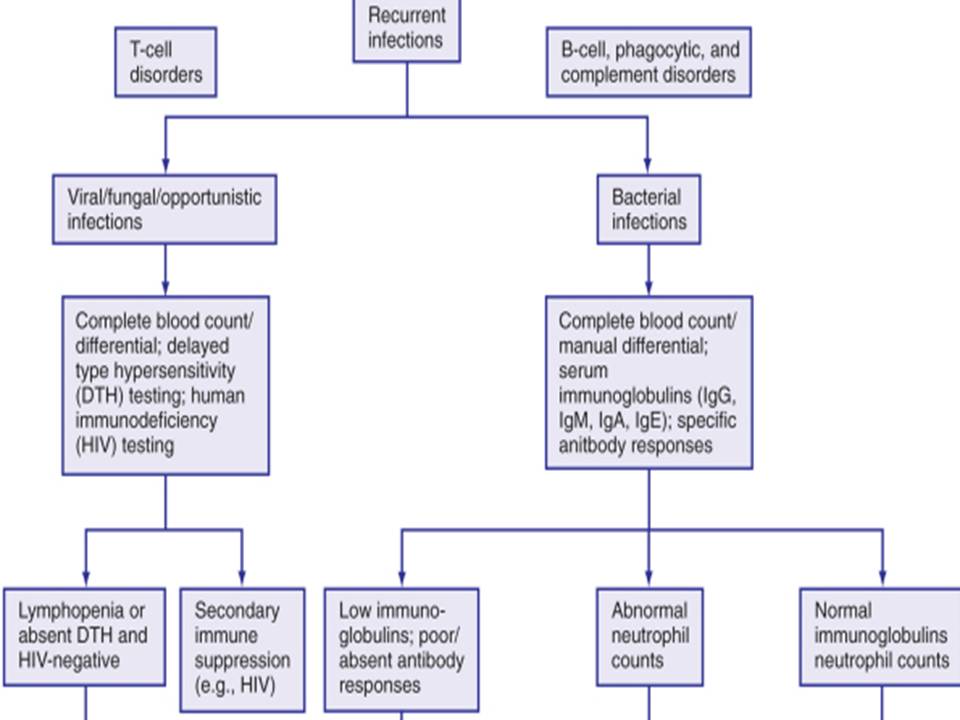
Recurrent Infections
Evaluation
History
Physical examination
Family History
Investigations
Serum IgM : Low & Neutropenia
Serum IgA, IgG : Normal
Differential Diagnosis Of Febrile neutropenia
Infection
30-40%
Malignancies 20-25%
collagen-vascular disease
10-20%
Miscellaneous 15-20%
drugs (barbiturates, antibiotics, antihypertensives, antiarrhythmic, phenytoin,
antihistamine, salicylates, cimetidine, bleomycin, allopurinol),
Factitious,….
Undiagnosed 10-15%
Initial Evaluation in Fever/Neutropenia
ENT(sore throat)
Dental sepsis
Mouth ulcers
focus on lungs,
perirectal region (no rectal exam)
Skin sores (gluteal Abcess)
GI
Laboratory examination:
CBC, diff (biCytopenia)
U/A:NL, U/C:Neg
blood cultures: Neg
PBS
ESR (increased)
CXR
LP
wound cultures when appropriate ??
Differential Diagnosis Of Febrile neutropenia
Infection
30-40%
Malignancies 20-25%
collagen-vascular disease
10-20%
Miscellaneous 15-20%
drugs (barbiturates, antibiotics, antihypertensives, antiarrhythmic, phenytoin,
antihistamine, salicylates, cimetidine, bleomycin, allopurinol),
Factitious,….
Undiagnosed 10-15%
Malignancies commonly associated with Fever
Hodgkin’s disease
Non-hodgkin’s lymphoma
Renal cell carcinoma
Hepatoma
Colon carcinoma
Atrial myxoma
Leukemia
Diagnostic Testing
ESR
If elevated →
significant inflammatory process
Greatest use in establishing a serious underlying disease, … esp. if v. high
→
ESR > 100 mm/h
Differential Diagnosis Of ESR Rising
ESR esp. if v. high →
ESR > 100 mm/h
is elevated in:
Bacterial Infection( Tuberculosis)
Neoplasm
Immunological-mediated inflammatory states
( m myeloma \ temporal arteritis )
Differential Diagnosis Of Low IgM
Multiple Myeloma
Some inherrited immune disease
Some types of Lukemia
Lukemia
ALL 77%
AML 11%
CML 2-3%
JCML 1-2%
Clinical Manifestations
Anorexia
Fatigue
Irritability
Intermittent Low grade Fever
Thrombocytopenia 75%
Hepatosplenomegaly 30-40%
CNS symptoms 5%
Diagnosis
Bone Marrow Aspiration
Don’t Forget
Early Diagnosis
دکتر سید رامین
مدنی
رزیدنت بیمارستان امام حسین
IN THE NAME OF GOD
History of patient
The girl, 2y
:
1th hospitalization:
prolonged fever, neutropenia, high ESR
2th
hospitalization:
fever,
gloteal abscess,hepatomegaly, neutropenia, anemia, thrombocytopenia,high ESR,
low IgM, high LDH
3th hospitalization:
fever,partial seizure, brain lesion(abscess), anemia, high ESR, chest
infiltration
The following features should lead to suspicion of an immunodeficiency
• Six or
more new infections within 12 months
• Two or
more serious sinus infections or pneumonias within one year
• Two or
more episodes of sepsis or meningitis
• Two or
more months of antibiotics with little effect
•
Need for intravenous antibiotics and/or hospitalization to clear infections
•
Failure to gain weight or grow normally
•
Resistant superficial or oral candidiasis
•
Recurrent tissue or organ abscesses
The following features should lead to suspicion of an immunodeficiency
•
Infection with an opportunistic organism
•
Complications from a live vaccine
• Family
history of immunodeficiency or unexplained early death
•
Unexplained autoimmunity
•
Lymphopenia in infancy
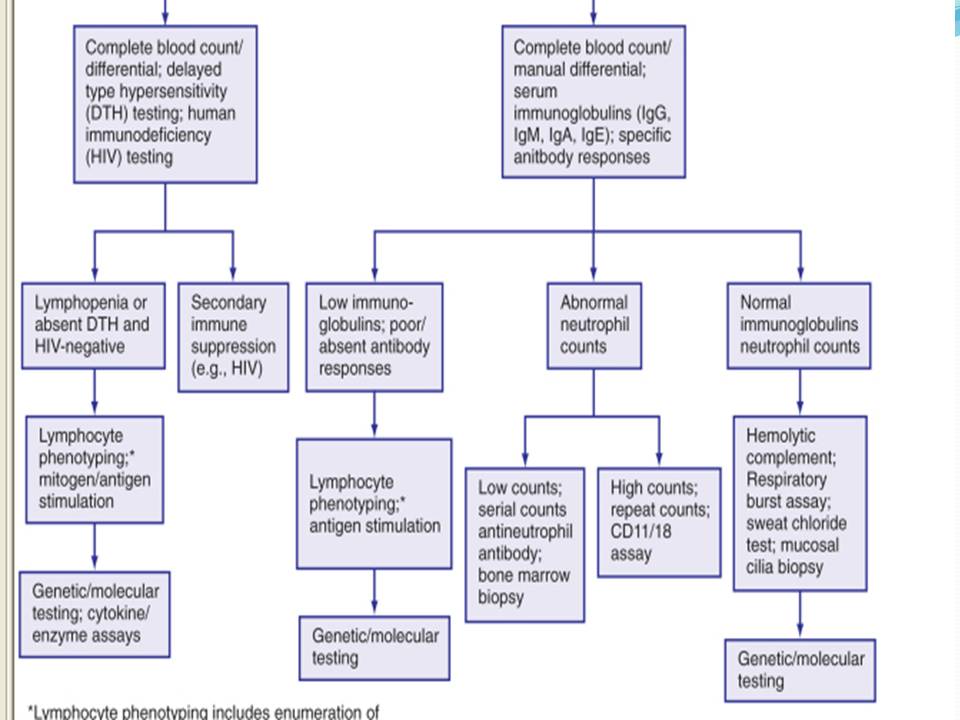
Immunodeficiency
Immunodeficiency may be
primary
or
secondary.
Secondary
immunodeficiencies usually occur well after infancy while most primary
immunodeficiencies are inherited and present during the first years of life.
Primary immunodeficiencies
overall incidence:
1 in 10,000
prevalence :1 in
2000 children
More than 150
disorders have been characterized.
Primary
immunodeficiencies most often affect B cell function.
The type and
pattern of recurring infections depend on which components of the immune system
are affected .
three-fourths of
the primary immunodeficiencies are caused by an antibody (B cell) deficiency or
a combined antibody plus cellular (T cell) abnormality
Primary immunodeficiencies
Age of onset
Growth and
development
Immunization
history
PMH
Family history :
similar diseases,
recurrent infections,
unexplained death,
or autoimmune disease
Secondary immunodeficiencies
Secondary
immunodeficiencies are
more
common than
primary immunodeficiencies.
Over
50
disorders
leading to secondary immunodeficiency have been identified.
secondary
immunodeficiencies more often affect
T cells
(the
cellular system).
secondary immune
dysfunction leads to an increased incidence of infection and malignancy, and the
occurrence of autoimmune disease.Infection and malignancy can leads to
immunodeficiency.
Secondary immunodeficiencies
�
infection
Viral
infection
HIV,
AIDS
Measles
Herpes
viruses
Bacterial infection (superantigens)
Mycobacterial infection
Parasitic infection
fungal
infection
Secondary immunodeficiencies
Malignancy
Hodgkin's disease
Non hodgkin’
disease
leukemia(ALL,AML)
Solid tumors
Disorders of biochemical homeostasis
Diabetes mellitus
Renal
insufficiency/dialysis
Secondary immunodeficiencies
Hepatic
insufficiency/cirrhosis
Malnutrition
Autoimmune disease
Systemic lupus
erythematosus
Rheumatoid
arthritis
Trauma
Burns
Secondary immunodeficiencies
Immunosuppressive therapy
- Cytotoxic
chemotherapy for malignancy
- Treatment of
autoimmune disease
- Bone marrow
ablation prior to transplantation
- Treatment or
prophylaxis of graft vs. host disease
following bone
marrow transplantation
- Treatment of
rejection following solid organ
transplantation
Secondary immunodeficiencies
Environmental exposure
Radiation
Ionizing
Ultraviolet
Toxic chemicals
Other
Stress
Asplenia/hyposplenism
Allogeneic blood
transfusion
Positive findings
Prolonged fever
neutropenia
Hepatomegaly
anemia
Seizure
thrombocytopenia
Multiple lesions in
brain
high
LDH
abscess in two
organs
low IgM
Reccurent
infections
high
ESR
DDx:
1.Secondary
immunodeficiencies:
-
malignancy(pancytopenia,
rapid
onset, high LDH,
high ESR, hepatomegaly)
leukemia(
ALL, AML)
solid tumor(
with marrow involvment):
neuroblastoma, rhabdomyosarcoma
-
infection:
viral(
HIV )
bactrial
fungal ….
-
collagen vascular diseases
-
Drugs
Tanks for your attention
دکتر
نوید نمازی
رزیدنت بیمارستان شهدا
In The Name Of God
Case presetation
A 2 y/o girl was referred to our hospital with fever and right gluteal area pain
and swelling
18 days ago she had sore throat and a physician prescribed penicilline 6.3.3 IM
but her fever continued for 5 days and she was treated with ceftriaxone IV for 5
days in hospital
Laboratory tests were done
Lab tests
WBC: 11170 PMN: 12.7% Lymph:81%
Hb:12.8 Hct:33.9 MCV: 77.6
MCHC:37.8 RDW:11.7
PLT:279000
ESR:84
CRP:Negative
The fever discontinued during hospital admission and the patient discharged with
good condition
2 days later her parents noticed fever , inflammation and pain at injection site
and with diagnosis of abccess formatin , drainage was done in the hospital.
Laboratory test were done
Lab tests
WBC:13000 PMN:0% Lymph:93.2%
Hb:9.5 HCT:28 MCV:81.4
MCH:27.6 MCHC:33.9
PLT:77000
ESR:39 CRP:1+
BUN:10 Cr:0.6 Na:136 K:4.2
PT:12.5 PTT:21 INR:1
Past Medical History
First child , full term, no history of asphyxia and icter , her mother had no
history of miscarriage
she had an addmission because of diarrhea and vomiting few months before
No history of drug sensitivity
Parents are not related
Growth Indexes
Birth wt: 3500
HC:32 HL:50
2Yrs Wt: 12000 HC:47 HL:92
Vital signs
BP:110/90
PR:100
RR:28
AT:37.3
Physical Examination
The patient is conscious , not pale, not icteric
Head, neck, eyes, ears , nose and throat are normal
No deformity and retraction in chest exam and heart and lung ausculation is
normal
No lymphadenopathy , liver is palpated 2 cm below costal margin, no distension
in abdomen
Extrimities are normal
Other tests
PBS: Anisocytosis , Microcytic, Hypochrome, Ovalocytosis
CSF/A: WBC:0 RBC:0 Pr:23 LDH:205 GLU: 64 CSF/C: Negative
B/C: Negative U/C:Negative U/A:Normal
SGOT:13 SGPT:14 ALKP: 232
LDH:1859 serum IgM:Low
Chest X-Ray
Heart and mediastinum are normal
No infiltrative lesion in lungs
No pathologic finding in bones and soft tissue of thorax
Abdominal Ultrasonography
Liver is larger than normal (104 mm), intra and extrahepatic bile ducts, potal
and hepatic veins have normal diameter, gallbladder has normal wall thickness
and has no stone
Spleen has normal echo(110 mm) ,pancreas has normal diameter and echo
Left kidney(70mm) , Right kidney(62mm) , no lesin, stone, stasis, Bladder is
normal
Right gluteal area has no finding in favor of abcess , fat tissue around drain
is echogen
2 months later
Patient had fever and jerking movements in left limbs and left deviation in
eyes, without loss of conciosuness, 20 minutes duration , 2 times in a day
In neurologic examination, babinski sign was detected in left foot
Lab tests
WBC: 6000 PMN:53% Lymph:43%
Hb:9.2 MCV:88
PLT: 392000
PBS: Anisocytosis, Microcytic, Hypochrome , Poikilocytosis
Blood Biochemistry: Normal
ESR: 107 CRP: Negative
GALACTOMANAN(serum): Negative
Chest X-Ray
Paracardiac and parahilar opacity in right side and in lesser degree in left
side in favor of infectious infiltration
Brain MRI with/without contrast and Brain CT
Intra axial mass lesion with mild vasogenic edema and hemorrhage at right
frontal lobe
Prominency of brain sulci and ventricular system
No obvious midline shift
Multiple rim enhancing lesions in right frontal and left occipital lobe
First admission
Fever
Neutropenia (PMN=1418)
ESR:84
CRP :Neg
Second Admission
Fever+ Hypertension + Pancytopenia ( severe neutropenia)
+ LDH
BMB + BMA?
Third admission
Fever + Focal seizure
ESR :82( corrected ESR)
CRP:NEG
Bilateral Parahilar, paracardiac infiltration
Multiple rim enhancing lesions in brain imagings
Approach
Neutropenia
Infections
Sepsis
Drug
Auto immune (ANI)
Cyclic neutopenia
Schwachman - Diamond syndrome
Chronic neutropenia ( severe, benign)
GSD (type 1b)
Bone marrow infiltration ( Leukemia, Neuroblastoma, Rhabdomyosarcoma, Lymphoma)
Multiple Ring Enhancing Lesions
Fungal and parasitic infections
Metastasis
Primary Lymphoma
TB
Demyelinating disorders
Abccess
Immunodeficiency
+
Multiple brain lesions and lung infiltration
Hematologic Malignancy?
Opportunistic infections?
Hematologic malignancy
Leukemia
Neuroblastoma
Lymphoma
Opportunistic infectionc
Toxoplasmosis
Aspergilosis
Candida
…………..



|
|
|
