|
پروفسور محمد حسین سلطان زاده
استاد
دانشگاه علوم پزشکی شهید بهشتی
متخصص کودکان ونوزادان
طی دوره بالینی عفونی از میوکلینیک آمریکا
دبیر برگزاری کنفرانس های ماهیانه گروه اطفال
دانشگاه علوم پزشکی شهید بهشتی
|
خانم دکتر
سهیلا خلیل زاده
عضو هیئت علمی دانشگاه
علوم پزشکی شهید
بهشتی
بیمارستان مسیح
دانشوری
به اتفاق اعضای
هیئت علمی
گروه کودکان
بیمارستان مسیح دانشوری
معرفی کیس:
دکتر صدر
خانم دکتر ناهید رادمنش
رزیدنت بیمارستان مفید
خانم دکتر لیلا بنی آدم
رزیدنت بیمارستان امام حسین
خانم دکتر صدیقه تهرانچی
رزیدنت بیمارستان لقمان
خانم دکتر ندا قیام
رزیدنت بیمارستان شهدا
دکتر غفاری پور
فلو ریه بیمارستان مفید
دکتر کاکوئی
رادیولوژیست
بیمارستان مسیح دانشوری
خانم دکتر آقاخانی
رزیدنت
پاتولوژی
بیمارستان مسیح دانشوری
|
خانم دکتر آقاخانی
رزیدنت
پاتولوژی
بیمارستان مسیح دانشوری
پاسخ :
تشخيص هاي افتراقي:

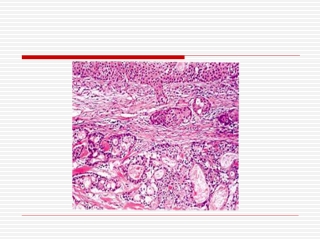
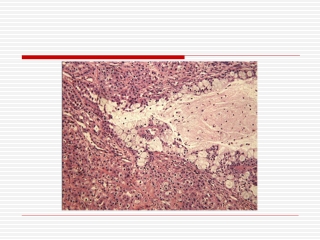
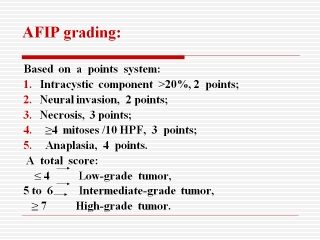
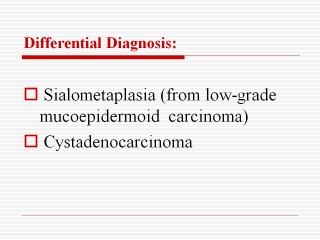
تشخيص نهايي
:
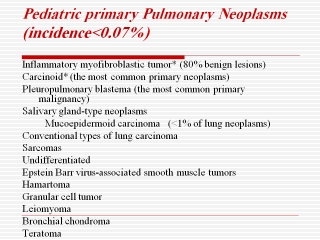
Low grade mucoepidermoid tumor
معرفی کیس:
دکتر صدر

تشخیص
های افتراقی:
خانم
دکتر ناهید رادمنش
رزیدنت بیمارستان مفید

خانم
دکتر لیلا بنی آدم
رزیدنت بیمارستان امام حسین
خانم دکتر صدیقه تهرانچی
رزیدنت بیمارستان لقمان

خانم دکتر ندا قیام
رزیدنت بیمارستان شهدا
دکتر غفاری پور
فلو ریه بیمارستان مفید

دکتر کاکوئی
رادیولوژیست
بیمارستان مسیح دانشوری

خانم
دکتر ناهید رادمنش
رزیدنت بیمارستان مفید

خانم
دکتر لیلا بنی آدم
رزیدنت بیمارستان امام حسین
خانم دکتر صدیقه تهرانچی
رزیدنت بیمارستان لقمان
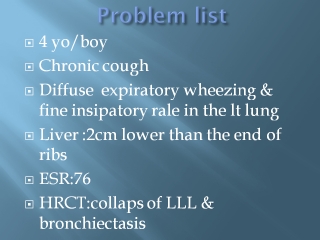
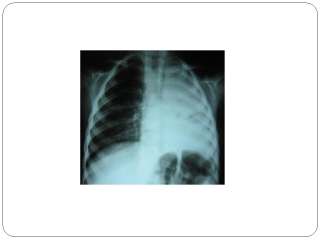
Problem list
Chronic cough
Acute respraitory distress
Anemia
Collapsed lung
Bronchiectasis&wheezing
hepatomegaly
Bronchiectasis
PATHOPHYSIOLOGY — In general,
induction of bronchiectasis requires two factors
An infectious insult
mpaired mucus clearance, airway
obstruction, or a defect in host defense
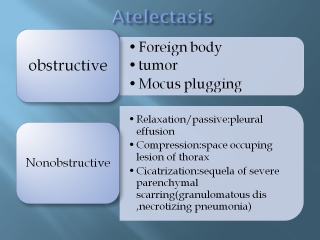
BRONCHIECTASIS
Definition: Abnormal
and permanent dilation of bronchi.
Focal or
diffuse distribution
Clinical
consequences – chronic and recurrent infection and
Pooling of
secretions in dilated airways.
Classification:
Cylindrical (fusiform)
Saccular
Varicose
The correlation of these patterns
with clinical status, etiology, or pathophysiology is not well established
.However, studies using high-resolution CT scan suggest that bronchiectasis may
be a dynamic process, and that cylindrical bronchiectasis can be reversible if
the underlying cause is successfully treated (eg, patients with atelectasis,
infection, or a retained foreign body)
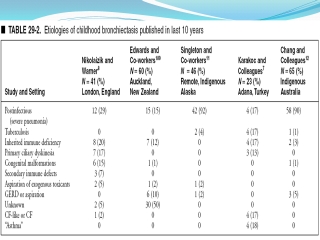
Etiology:
Acquired bronchial obstruction
Congenital anatomic defects
Immunodeficiency states
Abnormal secretion clearance
Infection
Other disorders (including alpha-1
antitrypsin, bronchiolitis obliterans, and connective tissue diseases)
in 25 to 38 percent of pediatric
cases, an underlying cause could not be identified despite a thorough evaluation
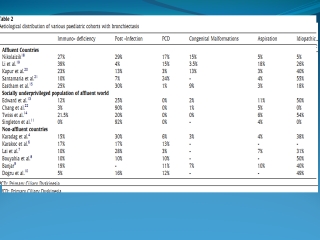
Causes of
bronchiectasis in children, based on distribution
Localized
Foreign body aspiration
Intraluminal obstruction
(granuloma, tumor)
Right middle lobe syndrome
Congenital abnormality (intralobar
bronchopulmonary sequestration, bronchial stenosis, bronchomalacia, tracheal
bronchus)
Extraluminal compression
(lymphadenopathy ie, tuberculosis or vascular compression)
Foreign body
aspiration
most common .a history of
choking may not be recalled. pneumonia may improve with antibiotic therapy.
However, the infiltrate on chest radiograph usually does not resolve, and
recurrence of pneumonia is common
TB
Pulmonary
disease and associated
intrathoracic adenopathy are the most frequent presentations of
tuberculosis in children
classic triad:
(1) recent close contact with an infectious case, (2) a positive TST, and (3)
suggestive findings on chest radiograph or physical examination
A negative TST does NOT
rule out tuberculosis disease. 15 percent or less for smear and 30 percent or
less for culture.The most common chest radiograph finding is a primary
complex, which consists of opacification with hilar or subcarinal
lymphadenopathy, in the absence of notable parenchymal involvement re.
Connective tissue
disorders&lung cancer
particularly
systemic lupus erythematosus (SLE), can be complicated by bronchiectasis
Wegener,sarcoidosis,churg-strauss syndrome
Congenital
Williams-Campbell syndrome
is a rare congenital disorder
characterized by deficient cartilage in the bronchial tree, causing generalized
tracheobronchomalacia .The bronchial cartilage is absent or deficient; the
segmental and subsegmental bronchi are dilated and collapse easily.
Children
typically present before three years of age with cough, wheezing, and
recurrent febrile illness
Congenital tracheobronchomegaly
(Mounier-Kuhn syndrome)
:a congenital disorder that is
characterized by markedly dilated trachea and main bronchi, resulting in dynamic
dilation and collapse during inspiration and exhalation. On pathologic
examination, there is atrophy or absence of elastic tissue, and thinning of the
muscular components of the airway. Outpouching of redundant mucosal tissue
results in pooling of secretions and recurrent infection, leading to
bronchiectasis. The clinical manifestations range from minimal disease to
respiratory failure and death
sequestrations
On a chest radiograph,
sequestrations typically appear as a uniformly dense mass within the thoracic
cavity or pulmonary parenchyma .Recurrent infection can lead to the development
of cystic areas within the mass disorder.
CT: solid mass that may be
homogeneous or heterogeneous, sometimes with cystic changes
Immunodeficiency
Bronchiectasis has
occasionally been reported in patients with selective IgA deficiency, which is
the most common immune deficiency
Abnl secretion clearance
Cystic fibrosis (CF)
is the most
common cause of bronchiectasis in industrialized countries. a persistent,
productive cough, hyperinflation of the lung fields on chest radiograph,
types:Classic,
Nonclassic CF
situs inversus (Kartagener
syndrome). Children
typically present with recurrent sinusitis, otitis media, and recurrent
pneumonia due to impaired ciliary function, and bronchiectasis
Young's syndrome is characterized
by obstructive azoospermia and sinopulmonary infections, but no
identifiable ciliary dysfunction or structural defec
Alpha-1 antitrypsin
Alpha-1
antitrypsin (AAT) is a protease inhibitor that protects tissues from
degradation. Severe deficiency of AAT is most often associated with emphysema
and cirrhosis. Bronchiectasis is an uncommon complication of
long-standing pulmonary disease; it may occur in older children and adults with
AAT deficiency
The main
clinical manifestations relate to three separate organs: the lung, the liver,
and much less often the skin.
severe
deficiency of AAT predisposes to chronic obstructive pulmonary disease,
especially panacinar emphysema. Within the first two decades of
life, liver dysfunction is the major threat to the health of affected
individuals, and pulmonary dysfunction is not a major concern
Persistent
bacterial bronchitis
(PBB) is increasingly recognized
as a cause of chronic wet cough, particularly in young children.
Identification and treatment of PBB is important because it may be a precursor
to chronic suppurative lung disease, including bronchiectasis
Childhood infections with
pertussis and measles have been associated with the development of
bronchiectasis .However, since the advent of routine vaccinations, the incidence
of these childhood infections has markedly decreased.
adenovirus
has been associated with the development of Swyer James syndrome, which is
characterized by unilateral small hyperlucent lung with bronchiectasis
and diminished arterial supply
missing
Developmental hx.
H.x of close contact for TB
Liver span
Bronchoscopy findings
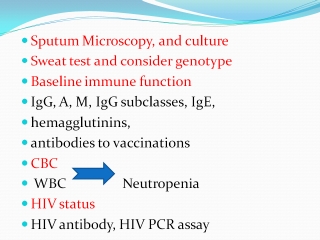
DIAGNOSIS
CF&TB
FBA&A1AT
خانم دکتر ندا قیام
رزیدنت بیمارستان شهدا

دکتر غفاری پور
فلو ریه بیمارستان مفید