|
CASE REPORT
Gastric Volvulus in Infancy
Presenting
With Pneumonia and Respiratory
Distress
Mohammad H.
Soltanzadeh , MD,ID
Professor of Pediatrics, Shaheed Beheshti
University
Of Medical Sciences , Tehran ,
IRAN
Manouchehr Davaie MD
Professor of Surgery , Shaheed
Beheshti University
Of Medical Sciences, Tehran , IRAN
ABSRACT
Gastric volvulus is an uncommon condition
more so in the Pediatric age group . The cause of gastric volvulus
may be idiopathic or secondary to various congenital or acquired
condition .In this study an 4-months old girl infant was admitted
for pneumonia and high fever and respiratory distress and agitation
Plain film and upper GI confirmed the diagnosis of gastric volvulus
with left – hemi diaphragmatic defects was treated successfully with
surgical intervention .
Key Words
: Gastric Volvulus,
Diaphragmatic defects , Organoaxial volvulus , Mesantroaxial
volvulus.
INTRODUCTION
Gastric volvulus is a rare condition. Over
300 cases have been reported since Berti first recognized this
condition in 1866, most of these were in adults (1)
Review of literature has revealed 116 cases
in infants and children up to 1994 (2)
In this condition , acquired torsion of
stomach results in partial or complete obstruction of its openings
and interruption of the blood supply .Early diagnosis and prompt
surgical intervention are required to avoid possible
complications.
CASE
SUMMARIES
An 4-months old girl infant was admitted to
the Pediatrics Ward in Imam Hossein Medical Center for pneumonia and
high fever and. Respiratory distress and agitation. Abdominal
distention and cyanosis frequently occurred after feeding .History
of infant shows one week before admission she received Antibiotic
due to pneumonia. She was delivered by normal vaginal delivery .
Her birth weight was 1750 gr. She admitted to Hospital After birth
due to cyanosis and respiratory distress about 10 days . After
discharge at time breast feeding she had cough and dyspnea and
cyanosis . History of epigastric distention on and off after feeds.
Routine vaccination has been done properly. Physical examination had
decreased breathing sounds in left hemi thorax and fine crackle no
other finding was noted in other side . Mild Fullness in
epigastrum and left hypochondrium T. 39/4c PR 170 RR 65 BP Normal .
Labotory finding : ESR Normal CBC and Diff Normal Hb .11 CRP
negative FBS, BUN, Electrolyte, Ca. and ABG about Normal Blood
Culture was Negative .
Chest X Ray and Upper GI series demonstrated
left postro- lateral Diaphragmatic Hernia . Spleen and stomach had
herniated up with Organoaxial Volvulus of stomach. Gastric Volvulus
with left Hemi Diaphragmatic eventration .Diaphragmatic defects
placation made a smooth recovery .


DISCUSSION
Gastric volvulus is defined as an abnormal
rotation of the stomach of 180 degree of one part of the stomach
around another (3) The normal stomach is fixed and prevented from
abnormal rotation by the four gastric ligaments . A normal
diaphragm also serves to prevent abnormal displacement of abdominal
viscera and gastric vovulus . ligamentous laxity , pyloric
obstruction leading to chronic gastric dilatation, hiatus hernia.
Other diaphragmatic hernias, eventration of diaphragm .
Abnormality of the suspensory ligament of
the stomach : gastrohepatic , gastrosplenic , gastrocolic ,
gastrophrenic usually long gastrocolic and gastrohepatic mesentery
classified as one of two types : Organoaxial or Mesenteroaxial.(4)
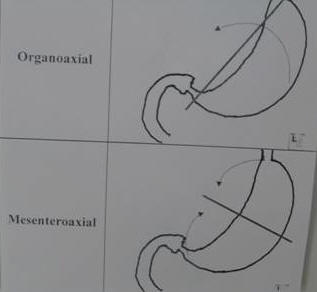
Organoaxial ; Twist
occurs along a line connecting the cardia and the pylorus – the
luminal (long) axis of the stomach. The antrum rotates in opposite
direction to the fundus of the stomach. Most common type , usually
associated with diaphragmatic defects , vascular compromise more
common . Strangulation and necrosis commonly occur with the type and
have been reported in 5-28% of cases.
Mesentroaxial ;
Twist occurs arounds a plane perpendicular to the luminal
(long) axis of the stomach from lesser to greater curvature, The
antrum rotates anteriorly and superiorly so that the posterior
surface of the stomach lies anterior . chronic symptoms more common
. Diaphragmatic defects less common.The rotation are usually
incomplete and occurs intermittently. Vascular compromise uncommon.
The clinical symptoms;
depend on the extent or degree of rotation and obstruction in
acute gastric volvulus . Time and need of surgical intervention
always determined by the evidence of vascular compromise . Severe
epigastric pain and distention , violent unproductive retching and
inability to pass a NG tube compromises the classical tiad of
Borchardt (5) . If vascular compromise occurs, there is 30%
mortality rate. The features result from obstruction at the cardia
and / or pylorus . Sawaguchi has attributed vomiting in young
infants to the mal development of hiatal function (6) .
According to etiology
; gastric volvulus can be classified as either type 1 (
idiopathic ) type 2 (congenital or acquired ) .
Imaging findings ; Massively
dilated stomach in LUQ possibly extending into chest . Inability of
barium to pass into stomach ( when obstructed ). Frontal radiograph
from an upper GI examination shows the stomach located in the lower
chest in a large hiatal hernia . The greater curvature of the
stomach lies superior to the lesser curvature in an organoaxial
twist . In the cases of mesentroaxial volvulus , gastric shadow may
show double air fluid levels in erect position with a
characteristic beak, one the fundus and the other in the antrum . In
organoaxial type , the stomach lies rather horizontally on plain
film with single fluid level without the characteristic beak.
Acute gastric volvulus is a surgical
emergency as delay in recognition and treatment can cause
strangulation and perforation of stomach.(7) .
In this case ; gastric volvulus with left
hemi- diaphragmatic eventration. Diaphragmatic defects placation
made as stomach recovery.
REFERENCES
1-
Berti A. Sigolar altorti glamento dell
esofagocol dudeno segitto da rapid morte . Gazz Med Ital prov ver
1866 ; 9: 139
2-
Amin M, Ei-Gohary , Atif Etiaby.
Gastric volvulus of the stomach. Am J Surg Int 1994 ; 9:486-488
3-
Tanner NC. Chronicand recurrent
volvulus of the stomach.Am J Surg 1968; 115: 505-515
4-
KamPui Fung. Gastric volvulus
complicating Nissen’s fundoplication J Pediatr Surg1990 ; 25:
1242-1243
5-
Borchardt M. Kur Pathologie and
therapie des magen volvulus . Arch Kin Chir 1904; 74: 243-260
6-
Sawaguchi S, Ohkawa H Kanmotsutt:
Idiopathic gastric volvulus in infancy and childhood . Z.Kinderchir
1981;32 : 218-233
7-
Bahasin DK,Nagi B ,Kochhar R
Endoscopic management of chronic organoaxialvolvulus of the stomach.
Am J Gastroenterol 1990 ; 85: 1486-1488
| 
