 |
M.H.Soltanzadeh ,M.D.,S.S.Nabavi,M.D.
Department of Pediatrics,Shahid Beheshti
University of Medical Sciences
Tehran,Iran
|
|
Introduction
The coexistence of achondroplasia and Klinefelter's syndrome is extremely rare. It would be of interest to note the effects of the two disorders and their recognition when occurring together .
Key words:Achondroplasia ,Klinefelter's syndrome
Case report
The child was an Iranian boy born in November of 1992 in Tehran .At the time that this report was being prepared he was 28 months old . Parents were normal with no history of achondroplasia and Klinefelter's syndrome or any other genetic disorder.
At the time of pregnancy ,the father was 41 years and mother was 30 years old .There was no history of consanguinity.
During the pregnancy ,sonography was done and the fetus was diagnosed to have a large head with a small body and limbs. After birth the finding of the sonography was confirmed.
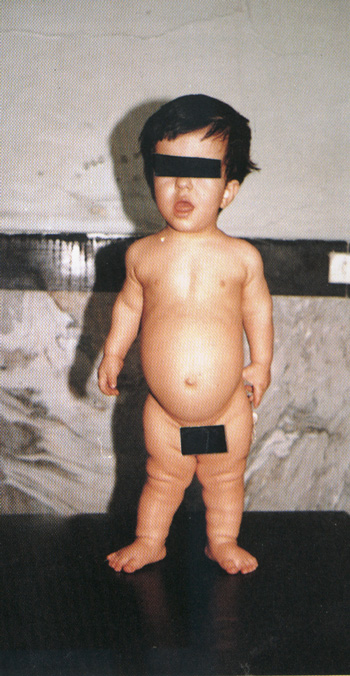
On physical examination the child had rhizomelic dwarfism, a large head with protruding forehead , mid facial hypoplasia , depressed nasal bridge , dental malocclusion , hypoplastic chin , low set ears, short neck and a decreased AP chest diameter .
The abdomen was protruding. There was evidenc of lumbar lordosis . The penis was small relative to the body ,2cm in length. The testes were present in the scrotum and seemed normal. Examination of the limbs showed short lower and upper limbs, specially in the proximal segment .
(Figure 1:The Patient's General appearance) Signs of trident hand was present. There were increased folds of soft tissue around the bones, positive waddling gate, the hands did not reach the greater trochanter while standing and there was bilateral genovarum.
Bow leg deformity was absent. Muscle tone was normal.
There were flexion contractures at the elbow joints, 35 degrees in the right and 30 degrees in the left elbow .Radiographic examination showed decreased interpedicular distances of the lumbar vertebrae. Form up downwards, body of the vertebrae showed anterior beaking and posterior scalloping. Sacro-coccyx was curved posteriorly with small square iliac wings and a horizontal acetabulum roof had champagne glass appearance. Sacrosciatic notch was small and narrow.
His IQ was normal. chromosomal analysis revealed 47XXY consistent with Klinefelter's Syndrome with no evidence of mosaicism (Figure 2). Routine laboratory investingations were normal . FSH was normal but LH was decreased (FSH=1.2, NL=0.5-12,LH=1.1,NL=2-17,estradiol=8.0,NL:0-100).
|
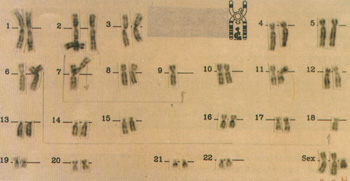
The Patient's Chromosomal analysis
Discussion
According to above mentioned findings ,Klinefelter's syndrome was diagnosed .The previous two case were diagnosed in teenagers but the age of diagnosis was lower in this case .
By a meticulous clinical examinations which was carried out on the child, it was found that the size of his penis was inappropriate for age, being smaller which itself is in correspondence with the diagnosis of Klinefelter's syndrome.
Another important point to be mentioned is the fact that in the coexisence of Klinefelter's syndrome, achondroplasia has an affect on patients height, causing shortness of stature, which suggests that Klinefelter's syndrome is not able to counter achondroplasia's effect on height and therefore if they coexisis, achondroplasia's effects on stature are more pronounced.
This patient was treated with growth hormone and limb lenghtening. Testosterone hormone therapy is suggested after the age of 11.
Refrences
1. Patton JT : Diagnostic Radiology : An Anglo-American text book of Imaging,vol.3, 2nd edition, Churchill Livingstone, 1992;PP:1647- 1650.
2. Sharrard WJW:Pediatric Orthopedics and Fractures, vo 1, 3rd edition, Oxford Blackwell Scientific Publication. 1993;PP:64-70.
3. Barr DGD, Goel KM: Forfar and Arneil's Text book of Pediatrics, Churchill Livingstone, 1992,PP:1647-50.
4. Silverman F: Caffey's Pediatric X-ray Diagnosis :an integrated imaging approach , vol2, Mosby , 1993;PP:1574-82.
5. Sillence DO, Behrman RE:Nelson Textbook of Pediatrics, 14th edition ,W.B.Saunders company ,1996:PP:1733-34;
6. Jones KL(ed):Smith's recognizable patterns of human malformation, 4th edition, W.B.Saunders Company ,1988;PP:66, 298-303, 698,704-5.
7. Nora J, Fraser FC:Medical Genetics:Principles and, Practice, 3th edition, Philadelphia, London , Febiger 1989,PP:63-64, 131.
8. Thomoson MW, et al : The Sex chromosomes and their abnormalities .In: Thompson & Thompson Genetics in Medicine, 5th edition ,W.B. Saunders Company , 1991 PP:239-40.
9. Okabe T, Nishikawa K, Mivamon C, et al :Promoting effects of human growth hormone in patients with achondroplasia . Acta Paediatr JPN. 1991;33(3):357- 62.
10. Mandoki MW , Summer GS:Klinefelter's syndrome:The need for early identification and treament. Clin Pediatr (Phila) 1991;30(3):161-4.
11. Kulakova TA , Ignatev IU: Achondroplasia with Klinefelter's syndrome. Klin Med (Mosk)1989;64(3)126-8.
12. Sayali BS, Gul D, Cakirbay H: Achondroplasia withxxy karyotype. Clin Genet 1994;45:217-218.
|
