Rickets
پروفسور محمد حسین سلطان زاده
استاد دانشگاه علوم پزشکی شهید بهشتی
www. ProfessorSoltanzadeh.com
Question?
oWhat
is Rickets?
Answer
o
Rickets
is the failure of osteoid to calcify in a growing child and this
is most commonly caused by a lack of vitamin D .
o
The adult equivalent is
osteomalacia.
Question?
oWhy
is Rickets reappearing ?
Answer
o
There has been an increase in
exclusive BF for prolonged periods without vitamin D
supplementation.
o
Human milk is low in vitamin D, &
AAP recommends vitamin supplementation for breast-fed Infants.
o
Reduced maternal sunlight
exposure reasons has become more common .
Question?
oWhat
is the best X-Ray view to obtain for evaluating possible
rickets ?
Answer
o
Anterior view of
the knee, incorporating femoral & tibial metaphyses and
epiphyses .
o
Bone growth is
most rapid in this area , and rachitic changes are seen earliest
at this location.
Question?
oWhat
X-Ray changes are noted in patients with rickets ?
Answer
o
Cupping ,
Fraying, & Irregularity of the metaphyses
.
o
Widening
of the physis as a result of
increased osteoid.
o
Loss or increased
separation of the zone of provisional calcification
.
Answer
oPeriosteal
reaction
oCoarsening
of trabeculae
oLoss
of bone density
oBowing
of long bones.
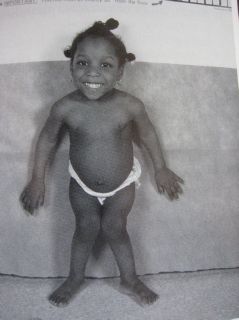
Question?
oWhat
are the physical signs that were suggestive of rickets ?
Answer
o
The anatomic
abnormalities of rickets result primarily from the inability to
normally mineralize osteoid
o
The bones become weak &
subsequently distorted .
Signs of rickets
include
o
Craniotabes
o
Femoral & Tibial bowing
o
Delayed suture & fontanel closure
o
“
Pigeon breast
“ sternal protrusion
as a result of use of accessory muscles
o
Frontal thickening
o
Detective tooth enamel
o
Harrison’s
groove
o
Palpably widened physes at wrists &
ankles
o
“ Rachitic Rosary
“enlarged
costocondral junctions
Rickets
o
Bone consists of protein matrix
called osteoid and mineral phase , principally composed of Ca &
Phosphate ,mostly in the form of hydroxyapatite
o
Osteomalacia is present when there
is :
o
Inadequate mineralization of Bone
osteoid
o
It occurs in children or adults
o
Rickets is under
mineralization of the cartilaginous epiphyseal growth plate
resulting in excessive accumulation of un mineralized matrix
(osteoid)
o
Rickets is seen only a
childhood because the growth plate exists only when the skeleton
is growing
o
Because growth plate
cartilage and osteoid continue to expand
o
But mineralization is
inadequate , the growth plate thickens
o
Also an increase in the
circumference of the growth plate and the metaphysis
o
This increases bones width at the
location of the growth plates .
o
Causing some of the classic
clinical manifestations such as :
o
Widening of the wrists and ankles
o
There is softening of the bones
that causes them to bend easily when subject to forces such as
weight bearing or muscle pull
o
This leads to a variety of bone
deformity
o
Osteomalacia
is under mineralization after growth is completed and is seen in
adults
o
اصولا ریکتز در اثر کمبود ویتامین
D
است
o
ناتوانی در مینرالیزه کردن استئوئید استخوان در حال
رشد است
o
تشکیل استخوان جدید توسط استئوبلاست ها شروع می شود
که مسئول رسوب ماتریکس و به دنبال آن مینرالیزاسیون آن هستند
o
استئوبلاست ها کلاژن ترشح می کنند وبعد از آن
تغییراتی در پلی ساکارید ها، فسفولیپید ها ، آلکالن فسفاتاز و
پیروفسفاتاز رخ میدهدتا مینرالیزاسیون رخ دهد
o
فاکتور های متعددی بر رشد استخوان تاثیر می گذارند
، کلسیم ، فسفر ، فلوراید ، هورمون رشد
oدر
ریکتز نقش رشد استخوان از تاخیر یا سرکوب رشد طبیعی غضروف اپی فیزی
وکالسیفیکاسیون طبیعی استخوان ناشی می شود
oاین
تغییرات حاصل کمبود نمک های کلسیم وفسفر موجود در سرم میباشد
oسلول
های غضروفی نمیتوانند چرخه طبیعی تکثیر ودژنراسیون خود را تکمیل
کنند
oنتیجه
این فرایند ایجاد یک خط اپی فیزی مضرس نامنظم در انتهای تنه
استخوان است
oشکست
در مینرالیزاسیون ماتریکس استخوان وغضروف به ایجاد یک بافت نرم ،
مضرس ، نامنظم منجر می شود
که مسئول بسیاری از ناهنجاری های اسکلتی ریکتز است
oریکتز
ناشی از کمبود ویتامین
D
است میتوان به عنوان تلاش بدن در جهت حفظ سطح سرمی کلسیم در نظر
گرفت
oدر
غیاب ویتامین D
کلسیم کمتری از روده جذب می شود
oبا
کاهش کلسیم پاراتورمون ترشح می شود
oاین
پدیده به حرکت در آمدن کلسیم وفسفر از استخوان منجر می شود
بنابراین غلظت سرمی کلسیم حفظ میشود
oدر
نتیجه غلظت پائین فسفر سرمی (به علت اینکه پاراتورمون باز جذب فسفر
را از کلیه کاهش می دهد )
oافزایش
فسفاتاز سرم ( ناشی از افزایش فعالیت استئوبلاستیک ) میباشد
o
آلکالن فسفاتاز سرم افزایش مییابد در شیرخواران
کمبود پروتیئن یا روی ممکن است طبیعی باشد
o
هموستاز کلسیم وفسفر به جذب روده ای کلسیم وفسفر
موجود در رژیم غذائی بستگی دارد
o
اگر محتوای روده اسیدی باشد
o
اگر شکر موجود در رژیم غذائی لاکتوز باشد
o
جذب کلسیم بیشتر میشود
o
فیتات موجود در حبوبات ممکن است جذب کلسیم را کم
کند
o
آهن موجود در رژیم غذائی ممکن است جذب فسفر را کاهش
دهد
o
اسید پالمیتیک واسیداستئاریک در رژیم غذائی جذب
کلسیم را کاهش می دهد
Etiology
o
There are
causes of rickets
including :
o
Vitamin D
disorders
o
Calcium deficiency
o
Phosphorous
deficiency
o
Distal renal tubular acidosis
o
Deficiency of metabolites of
vitamin D:
o
a. Sunshine deficiency
;
o
* Inadequate exposure to
sunlite
o
* Factors preventing
ultraviolet (UV) light penetration( industrial pollution ,
darkly pigmented skin, abundant clothing )
o
b. Dietary vitamin D deficiency
;
o
* Exclusive breastfeeding without
vitamin D supplements
o
* Food faddism (e.g. strict vegan
diet usually combined deficiencies of vit D and Ca are seen
o
c. Fat mal absorption
(usually causes deficiencies of both vit D and Ca)
o
* Celiac disease
o
* Extra hepatic biliary atresia
o
* Short bowel syndrome
Vitamin D
physiology
o
Vitamin D can be synthesized in
skin
o
Depend on the conversion of
7-dehydrochlestrol to vitamin D3 (3-cholecalciferol ) by
ultraviolet B radiation from the sun.
o
Vitamin D receptors are found on
the kidney, intestine ,bone osteoblasts ,parathyroid gland.
Vitamin D deficiency
o
Vitamin D2 is available in the
diet.
o
Cholecalciferol (vitaminD3)is
naturally presentin human skin in provitamin form
o
Vitamin D2&D3are hydroxylated in
the liver(25-Hydroxylation) to form (25-Hydroxylation) to form
25(OH)D3(calcidiol)
o
And again in the renal cortical
cells (1-hydroxylation) to produce 1,25-(OH)2D3 (calcitriol)

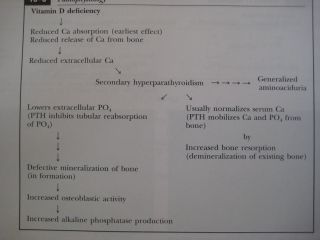
Pathophysiology
o
The main function of vit
D-parathormone (PTH)-endocrine axis is to maintain the extra
cellular fluid concentration of Ca & Ph (PO4) at appropriate
levels to permit mineralization.
o
The normal
critical product of serum Ca X PO4 concentration, each measured
in mg per deciliter , is 40 ; rickets occurs when the product
of CaXPO4 less than 30
Clinical manifestations
o
Craniotabes,
a softening of the cranial bones
o
Can be detected by applying
pressure at the occiput or over the parietal bones .
o
The sensation is similar to
the feel of pressing into a Ping-Pong ball and the
releasing
o
Craniotabes,
may also be secondary to;
o
Osteogenesis imperfecta
o
Hydrocephalus
o
Syphilis
o
It is a normal finding in
many newborns but it typically disappears within a few months of
birth .
o
Widening of the costocondral
junction ,
o
Results in a
Rachitic Rosary ,
o
This feels like the beads of
rosary as the examiners fingers move along the costochondral
junctions from rib to rib


Growth plate widening is also
responsible for the enlargement at the wrists and ankles .

o
The horizontal depression along the
lower anterior chest known as ;
Harrison Groove
occurs due to pulling of the softened ribs by the diaphragm
during inspiration

o
There is some variation in the
clinical presentation of the rickets based on the etiology .
o
Changes in the lower
extremities tend to be the
dominant feature in X-linked hypo phosphatemic rickets .
o
Symptoms secondary to hypo calcemic
occur only in those form of rickets associated with decreased
serum Ca
o
Many children present because of
skeletal deformity (Knock knee & Bow
leg)
o
Others may have difficulty
walking due to a combination of deformity & weakness
o
Other common presenting complaints
include F.T.T.&
symptomatic hypo calcemic
o
Characteristic rachitic changes can
be seen at other growth plates .
o
Decreased calcification lead to
thickening of the growth plate
o
The edge of the metaphysis loses it
sharp border, described fraying
o
Metaphysis changes from a convex or
flat surface to amore concave surface , this is termed
Cupping
seen at the distal end of
o
Radus, ulna, fibula





Diagnosis
Most cases of rickets are
diagnosed based on the presence of classic X-Ray abnormalities .
The diagnosis is supported by physical examination findings and
history and Lab test results that are consistent with specific
etiology
A
normal PTH level almost never occurs with vit.D deficiency and
o
Suggests a primary phosphate
disorder
o
Ca deficiency may occur with or
without vit.D deficiency
Nutritional
deficiency
o
The initial evaluation should
focus on :
o
Dietary history
o
Emphasizing intake of vitamin D &
Ca
o
Rickets has occurred in children
given product Soy milk but are deficient in vitamin D &
or minerals .
Rickets is seen in infants who are exclusively
Breast –fed.


Nutritional Rickets
o
Lab test:
o
Ca low or N
o
Po4 low for age
o
Alkaline phosphatase
elevated
o
PTH elevated
o
Calcidiol decreased
o
Calcitriol decreased, N ,or
elevated
o
Urine generalized
aminoaciduria
Mal absorption of vit. D
o
Is suggested by a history of
:
o
Liver or intestinal disease
o
Undiagnosed liver or intestinal
disease
o
Should be suspected if the has GE
symptoms
o
Occasionally , rickets may be in
Fat Mal absorption
Renal disease
o
A history of renal disease :
proteinuria, hematuria, UTI is an additional consideration ,
given the importance of CRF as a cause of rickets
Polyuria may occur in children with CRF or
Fanconi
syndrome


Children with
rickets
o
May have a history of :
o
Dental caries
o
Poor growth
o
Delayed walking gait
o
Pneumonia
o
Hypo calcemic symptoms
Family history given
Genetic cause


Congenital rickets
o
When there is severe
maternal vit D deficiency during;
o
pregnancy
o
Poor dietary intake of
vitamin D
o
Lack of adequate sun
exposure
o
Closely spaced pregnancies
o
This newborn with
rachitic changes
Secondary vitamin D
deficiency
o
inadequate absorption
o
Decreased hydroxilation in
the liver
o
Because
vitamin D is fat soluble
, variety of liver ,GE disease
, liver disease , cystic fibrosis
,celiac , crohn disease ,mal absorption
Treatment
o
Children with nutritional
vit D deficiency should receive vit
D &
o
Adequate nutritional intake of
Ca& Ph
o
There are 2 strategies for
administration of vitamin D
o
With stoss therapy,
300,000-600,000 IU of vit.D are administered orally or IM as
2-4 doses over 1 day
o
The alternative is daily, high dose
vit D
o
With doses ranging from 2,000
-5,000 IU /d over4-6 wk.
o
Followed by daily vit D 400 IU
/d
o
It is important to ensure that
children receive adequate dietary Ca
&Ph
o
this is usually provided by milk,
formula, & other dairy products

|

